 Skip to content
Skip to content Has this article been insightful? Share it!
A traumatic spine injury is any traumatic injury that damages the spinal cord, leading to a temporary or permanent change in neurological function, including paralysis. These injuries have a significant impact on the physical, mental and social well-being of the patients.
The spine serves as the primary axial backbone that protects the spinal cord and nerve roots. Any injury or impact in the spine has the potential to cause damage to both the bony spine and the spinal cord. The type of injury and the severity of the initial impact on the spine will determine the extent of spinal cord damage and skeletal injuries.
The main spine bone is connected to both the upper and lower limbs for mobility, along with a series of ribs for respiratory movement. Hence, a traumatic spine injury can result in the loss of many vital bodily functions such as sense and movement, respiration and breathing, blood circulation, blood pressure, bowel movement, as well as bladder control. Therefore, the extent of damage can be either neurological or bony structure-related with instability.
There are two types of neurological damage in traumatic spine injuries related to the spinal cord:
A complete loss of function (paralysis) on both sides of the body below the level of injury. It can be further classified into two sub-types:
• Quadriplegia: Paralysis of all four limbs
• Paraplegia: Paralysis in the lower half of the body
Following the injury, some function remains on one or both sides of the body as there are still certain pathways that allow communication between the brain and body.
Structural damage to the spinal axial bone, such as cracks in the vertebral body or fractures in facet joints with ligament injuries, can result in either a stable or unstable spine injury. Unstable spine injuries are more dangerous for the patient and put them at risk of neurological deficits. Therefore, any suspected spine injury patient should be carefully managed, and the patient should be transported to the nearest accident and emergency department by trained paramedics.
Depending on the location and severity of the injury, the damage may cause:
The symptoms people experience can vary depending on the type of injury, the level of the affected spinal cord and the extent of damage in the nerve fibres and tracts in the spinal cord.
If you experience significant trauma around your head or neck area, it is advised to visit the emergency room immediately to seek a medical evaluation for traumatic spinal injuries. It is always safer to presume that there is an injury until proven otherwise.
It is important to note that some traumatic spine injuries do not present immediate symptoms, especially those involving stable spines. The loss of sensation, progressive weakness, and other symptoms may occur gradually. If not attended to or treated by medical personnel, this could worsen and develop into more severe neurological deficits. This, in turn, will influence the anticipated extent of recovery.
The spinal cord plays a critical role in allowing us to perform our basic functions. If you suspect any trauma around your spinal cord, it is best to obtain a definitive diagnosis.
There are multiple causes of traumatic spine injuries, including:
If left untreated, the injury could progress in severity with further complications. As the spinal cord plays a vital role in controlling your nerves and muscles, an untreated spine injury may lead to:
When you are brought to the emergency room with signs of traumatic spine injury, the first thing your doctor would do is to ensure that the injury does not affect your breathing and heart rate. Following that, the doctor would assess how well your spinal cord and nerve roots are working by performing a thorough neurological examination to check:
Ability to move parts of your body (motor)
Ability to feel touch and sensations (sensory)
Ability to balance the body
Ability to control your bladder and bowel sphincters
Once you are stabilised, further tests will be carried out to evaluate the location and extent of your injury.
Imaging tests commonly used in diagnosing traumatic spine injury include:
A non-invasive X-ray imaging test that provides detailed 3-dimensional images of the spine vertebral bodies and their relation to the spinal cord and nerve roots, as well as the alignment of the spine. It is used to identify the type of fracture in the broken bones as well as the presence of blood clots or blood vessel damage with contrast.
A non-invasive test that utilises a magnetic field to visualise the detailed anatomy and underlying pathology of the spinal cord, nerve roots, ligaments and soft tissues along the spine.
Depending on your condition, you might also be sent for:
The first line of treatment for a traumatic spine injury involves spinal nursing, which entails immobilising the fracture with the unstable spine to prevent further neurological damage to the spinal cord and nerve roots. Immobilisation stabilises your spine using stiff neck collars or spinal nursing with skeletal traction and other external braces, such as a Halo vest.
However, in more severe cases, immediate spinal cord injury treatment may involve decompression and instrumentation via either open or minimally invasive surgery. This addresses spinal cord damage from broken bones, removes blood clots, and repairs damaged tissue.
After the surgery, it is critical to optimise blood flow to the spine while closely monitoring and evaluating neurologic function. Proper analgesics and corticosteroid injections help reduce the swelling in the spinal cord and relieve pain.
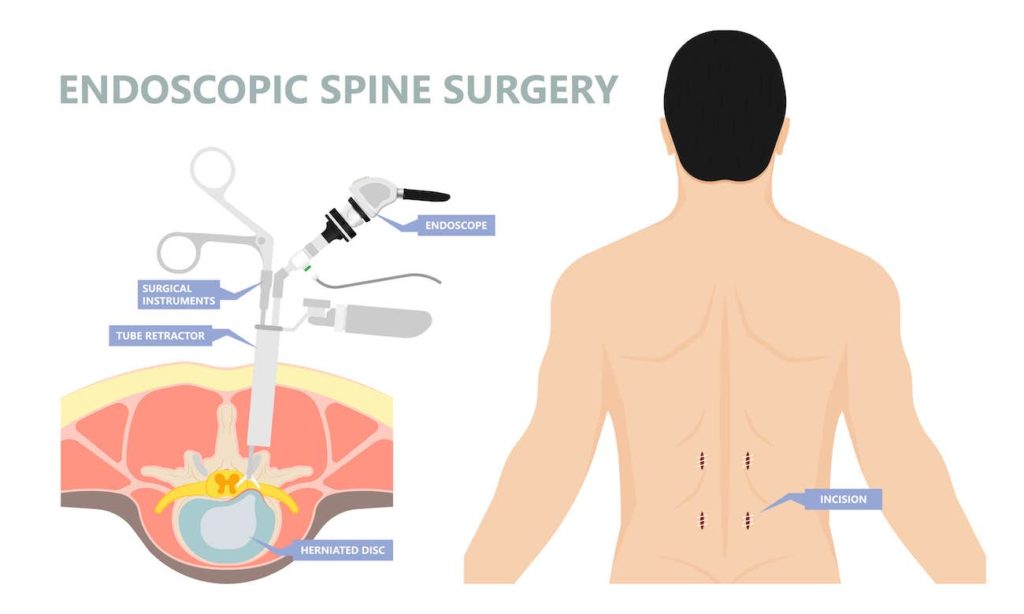
Minimally invasive spine surgery, or MISS, is a surgical procedure that uses specialised instruments and tiny incisions. Its main purpose is to treat spinal disorders while minimising the impact on nearby muscles and tissues. This technique includes a variety of procedures to treat diverse spinal conditions, such as endoscopic spine surgery and other treatments performed with needles or scopes through incisions that are usually less than 1 cm in size. With the use of smaller openings and specialised instruments, minimally invasive spine surgeries often accomplish effective results while minimising damage to muscles, spinous processes, ligaments, and tissues.
In minimally invasive surgery, the surgeon heavily relies on image guidance technology such as pre-and intraoperative 3D imaging, CAT scans, fluoroscopy, and intraoperative navigation. First, the procedure begins with creating small incisions directly over the pathological area. Then, instead of dissecting them like in open surgery, special retractors are utilised to dilate soft tissues and move muscles out of the way. In the end, sutures are used to close the tiny incisions made during minimally invasive spine surgeries. The reduced incision size also provides benefits such as faster recovery, less postoperative discomfort, and, in some cases, outpatient ambulatory care.

Depending on the severity of the injury, decompression surgery may be required:
Other possible treatments include:
Specific treatment would depend on a few factors:
A traumatic spine injury can affect a person’s basic function, directly impacting their quality of life and socioeconomic opportunities. If you have suffered head or neck trauma or are experiencing any of the symptoms listed above, it would be wise to seek medical attention from a neurosurgeon in Singapore.
Contact us today for an accurate diagnosis and treatment via minimally invasive spine surgery in Singapore.

Senior Consultant
Neuro & Spine Surgeon
MBBS, MSc Surgery, MRCS (Edin),
MMed. Sc (Gen Surg) (S'pore),
FRCS. Surgical Neurology (UK)
Dr Sein Lwin is an experienced Senior Consultant Neuro & Spine Surgeon and the Neurosurgical Director at the Advanced Brain and Spine Surgical Centre.
He is highly experienced in spine surgery and in minimally invasive approaches for spinal cord tumours and degenerative spine surgery. His specialised interests lie in endoscopic endonasal and open skull base surgery, pituitary tumours, vascular surgery, cranial nerve disorders and peripheral nerve conditions.
Many neurological conditions may require urgent attention. If you require immediate care, please contact us.
Contact Us For More Information
We provide quality specialised care for neuro and spine conditions.
For enquiries, leave a message and our friendly team will get in touch with you.
Monday – Friday: 9:00AM – 5:00PM
Saturday: 9:00AM – 12:30PM
Sunday & Public Holiday: Closed
We provide quality specialised care for neuro and spine conditions.
For enquiries, leave a message and our friendly team will get in touch with you.
Monday – Friday: 9:00AM – 5:00PM
Saturday: 9:00AM – 12:30PM
Sunday & Public Holiday: Closed
We provide quality specialised care for neuro and spine conditions.
For enquiries, leave a message and our friendly team will get in
touch with you.
Monday – Friday: 9AM – 1PM | 2PM – 5PM
Weekends & Public Holidays: CLOSED
Member of Beyond Medical Group
© 2023 All Rights Reserved | Advanced Brain & Spine Surgical Centre | Terms & Conditions
 Optimized by Seraphinite Accelerator
Optimized by Seraphinite Accelerator{kind=link}
{kind=link}