Your spinal cord carries signals back and forth between your brain and body, and is the thick bundle of nerves that runs from your brain down the inside of your spine. It is protected inside a tunnel in your spinal bones (vertebrae). A spinal cord tumour is an abnormal tissue growth in or around the spinal cord, and can be benign (non-cancerous) or malignant (cancerous).
Primary spinal tumours are tumours that originate in the spinal cord or its nerve fibres. They are relatively rare and majority are benign.
Some primary spinal tumours originate in the cells within the spinal cord or sheath of the nerve fibres, and when it grows, it compresses and expands the spinal cord and nerve roots as well as block the flow of CSF fluid pathway in the spinal cord, causing a fluid-filled cavity (syrinx) to form.
Primary spinal cord tumours could also originate in cells from the spinal cord and are gliomas, ependymoma and hemangioblastoma. If the tumour arises from the membrane of the spinal cord, it is a meningioma. Those arising from the nerve sheath or nerve fibres are either neurofibromas or shwannoma.
Abnormal connections between an artery and vein within the venous sinus wall, which is the tough covering over the brain or spinal cord.
The presentatioin of the spinal cord tumours are very variable. Some are asymptomatic when the tumour is too small but majority present symptoms such as pain at night. When the tumour grows large enough and compresses the spinal cord or nerve roots, the patient may develop neurological deficits, such as:
If you experience symptoms of a spinal cord tumour, visit a doctor promptly. If tumours are found to be compressing the spinal cord, they need to be treated as soon as possible to prevent irreversible damage, thus a doctor’s visit is advisable for early detection.
The development of spinal cord tumours is unclear, but researchers suggest that defective genes, either inherited or developed over time, play a role. Exposure to certain chemicals, viruses and autoimmune disorders could also cause spinal cord tumours.
Your doctor will conduct a complete medical history and perform general physical exams, neurological assessments and diagnostic tests in order to diagnose spinal cord tumours.
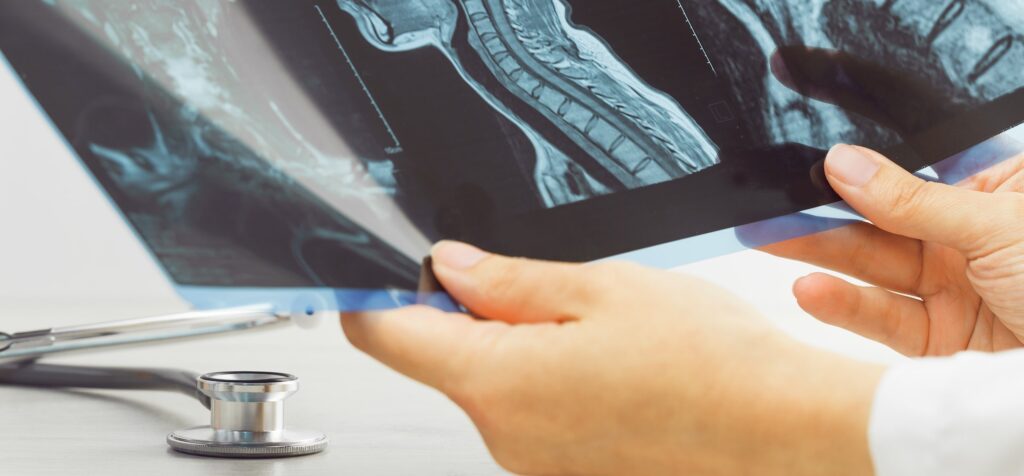
A powerful magnetic field and radio waves are used to allow viewing of the tumour’s structure, exact location and size in relation to the spinal cord. It is a mandatory investigation conducted for diagnosis of spinal cord tumours.
A CT scan is used to better visualise the vertebrae (bones of the spine) and other spinal structures and tissues to provide more information related to damage of the spine, and is also required for stabilisation of the spine after tumour removal.
In a CT myelogram, contrast dye is injected into the spinal column before a CT scan is taken for clearer viewing of the spinal cord, subarachnoid space, and other nearby structures. This test is useful for patients who are unable to undergo an MRI scan.
Full-body 3D images of the spine are created with the patient in a natural, standing position. An EOS scan emits much less radiation compared to CT scans and x-rays.
Low dose x-rays are used to measure bone density. If a spinal cord tumour is suspected to affect the strength of bones, a DEXA scan might be recommended.
A bone scan detects areas of increased activity in bone from a spinal cord tumour. A radioactive tracing material is injected intravenously and the patient is scanned to reflect changes in the bone.
A positron emission tomography (PET) scan produces images of organs and tissues and can measure vital functions, damaged organs and detect cancerous tumour cells to help gauge cancer spread.
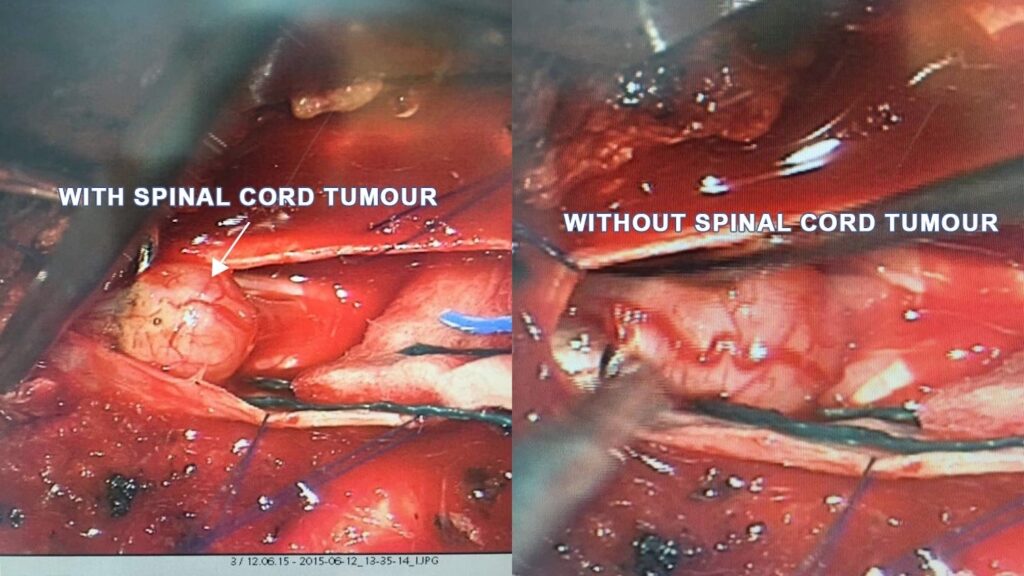
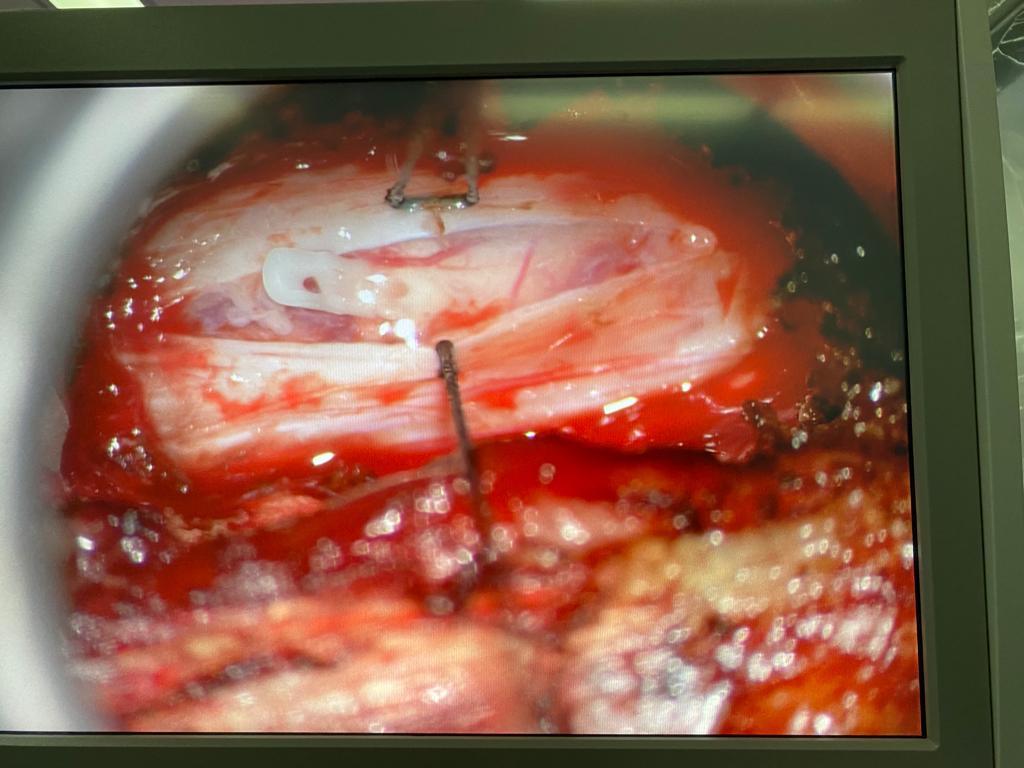
Surgery is often the treatment of choice for tumours that can be removed with an acceptable risk of spinal cord or nerve injury. Through the minimally invasive (keyhole) approach, small incisions are made and guiding instruments and microscopic video cameras are utilised to access tumours deep inside the body.
To minimise trauma during surgery, a tubular retractor is commonly used to progressively dilate the soft tissues, instead of cutting directly through the muscles and minimal bone exposure. An MIS approach can shorten your hospital stay, reduce post-operative pain and unnecessary instrumentation in the spine.
Spinal cord tumours could be primary tumours, where the abnormal tissue is often non-cancerous, or secondary tumours, which are cancerous. A spinal cord tumour can result in spinal cord compression, causing neurologic deficits and pain. Surgical treatment is usually recommended to preserve function and prevent irreversible damage.

Senior Consultant
Neuro & Spine Surgeon
MBBS, MSc Surgery, MRCS (Edin),
MMed. Sc (Gen Surg) (S'pore),
FRCS. Surgical Neurology (UK)
Dr Sein Lwin is an experienced Senior Consultant Neuro & Spine Surgeon and the Neurosurgical Director at the Advanced Brain and Spine Surgical Centre.
He is highly experienced in spine surgery and in minimally invasive approaches for spinal cord tumours and degenerative spine surgery. His specialised interests lie in endoscopic endonasal and open skull base surgery, pituitary tumours, vascular surgery, cranial nerve disorders and peripheral nerve conditions.
Many neurological conditions may require urgent attention. If you require immediate care, please contact us.
Contact Us For More Information
Your needs are important to us.
For enquiries, leave a message and our friendly team will get in touch with you.
Monday – Friday: 9:00AM – 5:00PM
Saturday: 9:00AM – 12:30PM
Sunday & Public Holiday: Closed
We provide quality specialised care for neuro and spine conditions.
For enquiries, leave a message and our friendly team will get in touch with you.
Monday – Friday: 9:00AM – 5:00PM
Saturday: 9:00AM – 12:30PM
Sunday & Public Holiday: Closed
We provide quality specialised care for neuro and spine conditions.
For enquiries, leave a message and our friendly team will get in
touch with you.
Monday – Friday: 9AM – 1PM | 2PM – 5PM
Weekends & Public Holidays: CLOSED
© 2023 All Rights Reserved | Advanced Brain & Spine Surgical Centre | Terms & Conditions